


Introduction: The effect of tyrosine kinase inhibitors (TKIs) on cognition in patients with chronic myeloid leukemia in chronic phase (CML-CP) is not well understood. Memory impairments have been reported in limited studies in CML patients on dasatinib and in gastrointestinal stromal tumor patients on imatinib, but additional research is needed. At our institution, we have observed that CML-CP patients spontaneously report new cognitive dysfunction (CD) while on TKIs. We sought to determine the prevalence of CD in CML-CP patients on TKIs, the TKIs associated with cognitive changes, and the management and outcomes of CML-CP patients with CD at our institution.
Methods: We performed a single-center, retrospective cohort study of active CML-CP patients in our Hematology clinic seen between January 2017 and December 2019. Patients were identified by ICD-10 codes and chart notes were reviewed for treatment course. Patients met criteria for CD if they reported new difficulties with cognition while on TKI treatment (as documented in the subjective or review of systems) and had no prior history of cognitive impairment. Descriptive statistics, Chi-square tests, and two-tailed t-tests were used to summarize the data.
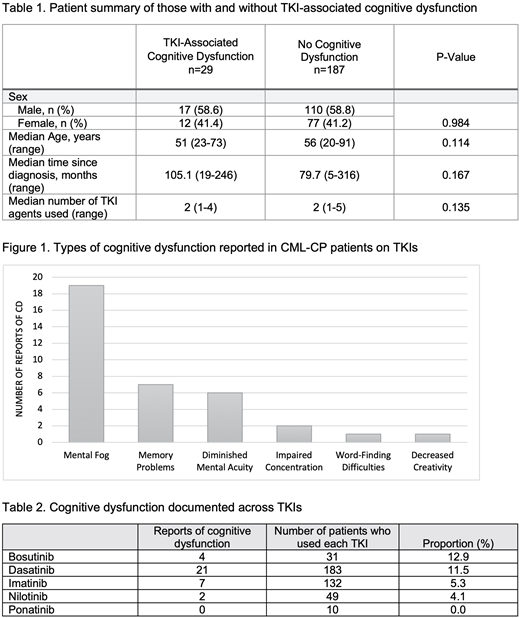
Results: We identified 216 CML-CP patients who were actively or previously treated with a TKI, with 29 patients (13.4%) reporting CD while taking a TKI. The median age for patients with CD was 51 years (range 23-73), compared to a median age of 56 years (range 20-91) in those without CD (P=0.114); there were no significant differences in sex (P=0.984) or in median time since diagnosis (P=0.167) (Table 1). The 29 patients generated 36 reports of CD, as 7 patients (24.1%) reported 2 types of cognitive changes while on TKI. The types of CD were documented as "mental fog" (n=19/36, 52.8%), memory problems (n=7/36, 19.4%), decreased mental acuity (n=6/36, 16.7%), problems with concentration (n=2/36, 5.6%), word-finding difficulties (n=1/36, 2.8%), and impaired creativity (n=1/36, 2.8%) (Figure 1).
Of the 29 patients who reported CD, 5 experienced it on 2 different agents, leading to 34 individual reports of CD. Among the 216 patients with CML-CP treated with TKIs, many used more than 1 agent: 31 used bosutinib, 183 dasatinib, 132 nilotinib, and 10 ponatinib. The percentage of CD reported in patients treated with each TKI was as follows: bosutinib 12.9% (n=4/31), dasatinib 11.5% (n=21/183), imatinib 5.3% (n=7/132), nilotinib 4.1% (n=2/49), and ponatinib 0% (n=0/10) (Table 2).
For management, 20.7% (n=6/29) underwent successful prescribed discontinuation, 27.6% (n=8/29) attempted discontinuation but resumed TKI after loss of MMR, 24.1% (n=7/29) underwent TKI dose reductions, 20.7% (n=6/29) changed TKIs, and 6.9% (n=2) had no change in management. In the 6 patients who successfully discontinued TKI, all but 1 (83.3%) reported complete resolution of their CD while off of TKI. For those who attempted discontinuation but had loss of MMR, 6 of 8 (75%) had documented improvement of CD off of treatment; after restarting TKI, CD returned in 5 patients (83.3%). Of the remaining patients who underwent TKI dose reductions (n=7), 1 patient had documented improvement of CD, 2 had no change, and 4 had unspecified outcomes. Of the patients who changed TKIs (n=6), 1 patient had documented improvement of CD, 4 had no change, and 1 had unspecified outcomes. In the 2 with no change in management, outcomes were not specified.
Conclusion: Cognitive dysfunction in CML-CP patients was reported with all first- and second-generation TKIs; the analysis of ponatinib was limited by small numbers. Bosutinib had the highest proportion of CD in our cohort, an association that has not been previously reported. Our analysis supports that TKI-associated CD is reversible since it resolved in 78.6% (n=11/14) patients when off of TKI during discontinuation. While 13.4% of our CML-CP patients had CD, due to spontaneous reporting and subtle presentation of cognitive impairment, the true prevalence of CD in CML-CP patients on TKIs is likely substantially higher. Future studies should involve prospective data collection of objective cognitive testing and patient reported outcomes in CML-CP patients for further evaluation of TKI-associated cognitive dysfunction.
Schoenbeck:American Society of Hematology: Research Funding. Smith:Sanofi: Honoraria; FujiFilm: Other: Research support, Research Funding; Revolution Medicines: Other: Research Support, Research Funding; Astellas Pharma: Honoraria, Other: Research Support, Research Funding; Daiichi Sanyko: Consultancy, Honoraria; Abbvie: Other: Research Support, Research Funding. Shah:Bristol-Myers Squibb: Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal